
Introduction
| In 1997,The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) developed an educational program entitled, “The Fundamentals of Laparoscopic Surgery” (FLS). FLS teaches the fundamental knowledge, judgment, and technical skills that were specific to laparoscopic surgery. FLS is comprised of a cognitive knowledge component, as well as a skills-based portion pertinent to laparoscopic surgery.The FLS program was first released as a CD ROM with two discs. Disc 1 includes the didactic information and Disc 2 includes a description of the manual skills. Disc one was organized into four chapters: pre-operative considerations, intra-operative considerations, basic laparoscopic procedures, and post-operative considerations. Each chapter contains learning objectives and self-study questions. Currently, an online version of the FLS material is available.The content of FLS is appropriate for surgical trainees as well as practicing surgeons. The FLS program remains one of the most rigorously studied, evidence-based surgical skills programs. FLS is CME accredited, and in 2008, the American Board of Surgery required FLS as a prerequisite of the ABS Certifying Examination. | 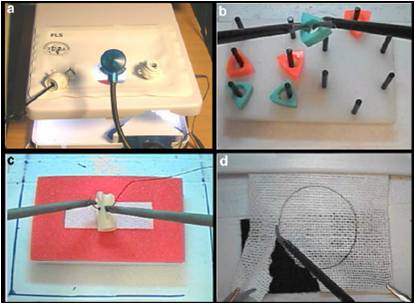 FLS Manual Tasks |
Cognitive Component
The cognitive curriculum is organized into four chapters: pre-operative considerations, intra-operative considerations, basic laparoscopic procedures, and post-operative considerations
Pre-operative considerations
The module on pre-operative considerations provides information on laparoscopic equipment, setup, and trouble-shooting. Energy devices are also covered in detail in respect to the science of hemostasis.
Intraoperative considerations
the intraoperative module includes the physiologic effects of pneumoperitoneum and carbon dioxide, including potential hemodynamic, metabolic, and respiratory complications. Safe trocar placement is also covered in this section.
Basic laparoscopic procedures
The basic procedure covered in FLS is the diagostic laparoscopy. This maintains the mission of FLS to be applicable to all subspecialties utilizing laparoscopy. Surveying the entire abdomen and pelvis, as well as methods of biopsy are covered. This section also details managing hemorrhage effectively during laparoscopic surgery.
Postoperative considerations
This module covers routine postoperative recovery as well as problems related to post-operative care, and describes the recognition and management of potential complications associated with access and exit, those that may be associated with pneumoperitoneum, and those related to specific interventions. The management of a patient following laparoscopic surgery is framed in the benefits of laparoscopy, including less incisional pain, and decreased incidence of ileus.
Manual Tasks
The goal of this section is to build the foundation for acquiring the technical skills upon which laparoscopic surgery depends. There are a series of skills that are distinct and specific for laparoscopic surgery and that form the fundamental basis for performance of a number of laparoscopic operations. These skills were defined by a group of practicing laparoscopic surgeons after first viewing videos of a variety of laparoscopic operations. They then listed those differences that distinguished the performance of laparoscopic surgery from the same operation done open. Once this list was generated, a series of exercises was created to teach and evaluate performance of these skills. In developing a program to teach and evaluate manual skills, one of the foremost goals was to create a simulation program that did not require the use of live animals, that was relatively inexpensive, allowed flexibility so that the learner could use instruments that he or she actually used within the operating room environment, and that was flexible enough to add additional exercises as people started to use this platform to develop specific skills for specific operations. Portability was another requirement that was encouraged in the development.
The FLS Manual Tasks include:
- PEG Transfer
- Pattern Cutting
- Endoloop Placement
- Extracorporeal Suturing
- Intracorporeal Suturing
The system that was incorporated in the FLS program was a derivative of the MISTELS (McGill Inanimate System for Training and Evaluation of Laparoscopic Skills) program originally developed at McGill University for this purpose. The underlying objectives of the manual skills module were to require a surgeon to work using a monocular optical system such as provided with standard laparoscopy, to manipulate instruments placed through a trocar, thus limiting the degrees of freedom of the instruments and creating a fulcrum effect that is the hallmark of laparoscopic surgery. Once developed, the specific tasks demanded that the surgeon use both hands in a complementary fashion to manipulate objects within a box covered by an opaque cover while performing a series of exercises of increasing difficulty. Metrics were designed for each task to provide objective measures of efficiency and precision, while penalizing specific errors. A score could then be assigned for performance of each task, and a total score was calculated y summing the normalized scores for the individual exercises. Scores were normalized to ensure that each task was scored within a similar range.
See Also
References
Please properly annotate all references
- Scott DJ. Ritter EM. Tesfay ST. Pimentel EA. Nagji A. Fried GM. Certification pass rate of 100% for fundamentals of laparoscopic surgery skills after proficiency-based training. [Article] Surgical Endoscopy & Other Interventional Techniques. 22(8):1887-1893, 2008
- Ritter EM, Scott DJ (2007) Design of a proficiency-based skills training curriculum for the Fundamentals of Laparoscopic Surgery. Surg Innov 14; 107, 2007.
- Swanstrom LL. Fried GM. Hoffman KI. Soper NJ. Beta test results of a new system assessing competence in laparoscopic surgery. Journal of the American College of Surgeons; 202(1): 62-9, 2006.
- Korndorffer Jr JR, Dunne JB, Sierra R, Stefanidis D, Touchard CL, Scott DJ. Simulator training for laparoscopic suturing using performance goals translates to the OR. J Am Coll Surg, 201:23 – 29, 2005.
- Stefanidis D, Sierra R, Markley S, Korndorffer Jr JR, Scott DJ. Proficiency maintenance: impact of ongoing simulator training on laparoscopic skill retention. J Am Coll Surg, 202:599 – 603, 2006.
- Stefanidis D, Sierra R, Korndorffer Jr JR, Dunne JB, Markley S, Touchard C, Scott DJ. Intensive CME course training on simulators results in proficiency for laparoscopic suturing. Am J Surg, 191:23 –27, 2006.
- McCluney AL. Vassiliou MC. Kaneva PA. Cao J. Stanbridge DD. Feldman LS. Fried GM. FLS simulator performance predicts intraoperative laparoscopic skill. [Article] Surgical Endoscopy & Other Interventional Techniques. 21(11):1991-1995, 2007
- Dauster B, Steinberg AP, Vassiliou MC, Bergman S, Stanbridge DD, Feldman LS, Fried GM: Validity of the MISTELS Simulator for Laparoscopy Training in Urology. J Endourol. Jun; 19:541-5, 2005.
- Fraser SA, Feldman LS, Stanbridge D, Fried GM: Characterizing the learning curve for a basic laparoscopic drill. Surgical Endoscopy, 19(12): 1572-8, 2005.
- Fried GM, Feldman LS, Vassiliou MC, Fraser SA, Stanbridge D, Ghitulescu G, and Andrew CG. Proving the value of simulation in laparoscopic surgery. Ann Surg 2004; 240: 518-528.