Carmen F Fong1, Joanne Ling2, David Pechman1, Steven Cai, MD1. 1Mount Sinai Beth Israel, 2CUNY Medical School
Background: The current teaching is that gallbladder polyps greater than 1cm need to be resected via cholecystectomy. Many of these polypoid lesions are benign on final pathology and the benefit of the patient undergoing surgery is unclear.
The literature suggests that 6.9-15.8% of Chinese patients will have gallbladder polyps, with a predilection towards males and those with positive hepatitis B surface antigen (Lin et al., 2008). Of 40 patients studied by Zhang in 1991, 23 (57.5%) had cholesterol polyps, 5 (12.5%) inflammatory polyps, and 4 (10%) had adenocarcinomas (Zhang, 1991). However, these studies were done in China in the 1990s, and no recent study of the Chinese-American population exists.
Methods: This is a retrospective chart review designed to study the rate of gallbladder neoplasms in a 3-surgeon practice based in downtown Manhattan. Using our office electronic medical records, we searched for cases with the CPT code for laparoscopic or open cholecystectomy (47562, 47563). We then searched for patients with the ICD-9/ICD-10 code for gallbladder polyp (575.6, K82.1). These cases were entered into an Excel database and the results were studied with SPSS statistical software.
Results: There were a total of 185 cholecystectomies performed by our practice between 2012-2016. 176 were laparoscopic cholecystectomies and 9 were open or lap-converted-to-open cases. Of these, 33.5% (62/185) were performed for gallbladder polyps. Only 1 case (1.6%) was found to have adenocarcinoma on final pathology. Combining adenoma/adenocarcinoma, the incidence of neoplasm is 12.9% (8/62). The remainder had cholesterol polyps or chronic cholecystitis.
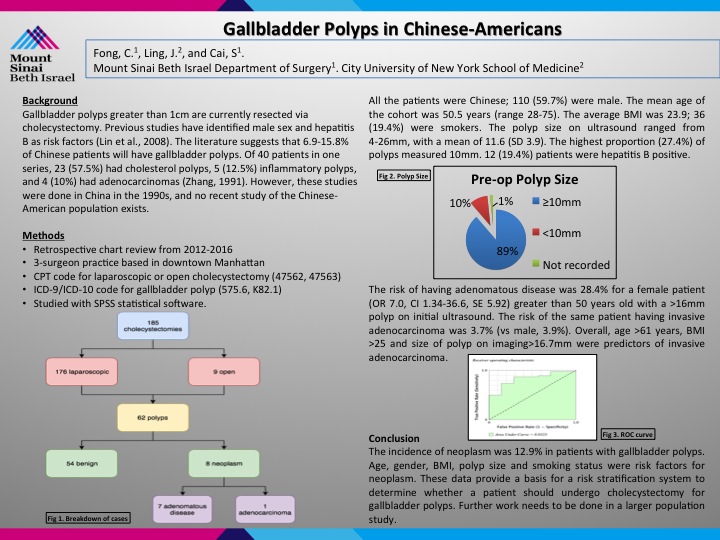
All the patients were Chinese. 59.7% were male. The mean age of the cohort was 50.5 years. The average BMI was 23.9. 19.4% were smokers. The polyp size on ultrasound ranged from 4-26mm, with the highest proportion (27.4%) being 10mm. 12 patients were hepatitis B positive (19.4%); the majority did not have hepatitis.
The risk of having adenomatous disease was 24.9% for a male patient (OR 8.76, p=0.04) greater than 50 years old with a >16mm polyp on initial ultrasound. The risk of the same patient having invasive adenocarcinoma was 0.02%. Overall, age >61, BMI >25 and size of polyp on imaging>20mm was more predictive of invasive adenocarcinoma.
Conclusion: We propose a risk stratification system based on age, gender, BMI, polyp size and smoking status to determine whether a patient should undergo cholecystectomy for gallbladder polyps.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 80568
Program Number: P090
Presentation Session: Poster (Non CME)
Presentation Type: Poster