Nikhil Panda, MD, Christopher R Morse, MD, David W Rattner, MD. Massachusetts General Hospital
Background: Approximately 3-6% of patients undergoing anti-reflux surgery require “redo” surgery for persistent gastroesophageal reflux disease (GERD). Further surgery for patients with two failed prior anti-reflux operations is controversial due to the morbidity of reoperation and poor reported results. We therefore examined our experience with surgical revision of patients with at least two failed anti-reflux operations.
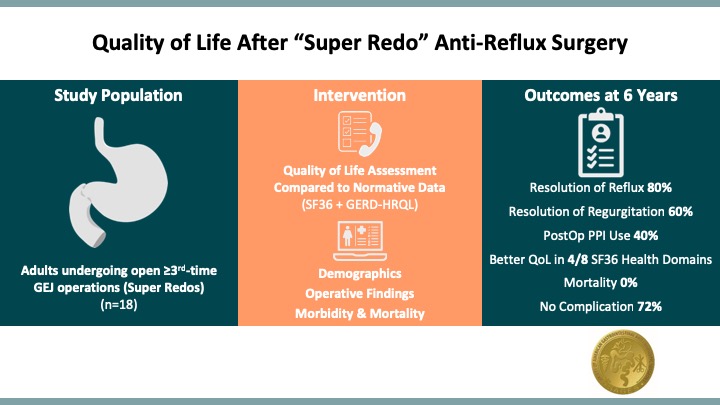
Methods: Adults undergoing at least a second-time revision anti-reflux operation between 1999-2017 were eligible. The primary outcomes were general and disease-specific quality of life (QoL) scores as determined by Short-Form-36 (SF36) and GERD-Health-Related-QoL (GERD-HRQL) instruments, respectively. Secondary outcomes included perioperative morbidity and mortality.
Results: We identified 18 patients (13 with 2 prior operations, 5 with 3 prior operations). All were followed for a median of 6 years [IQR 3,12]. Sixteen patients (89%) underwent open revisions (14 thoracoabdominal, 2 laparotomy) and 2 patients were revised laparoscopically. Indications for surgery were reflux (10 patients), regurgitation (5 patients), and dysphagia (3 patients). Intraoperative findings included mediastinal wrap herniation (9 patients), misplaced wrap (2 patients), mesh erosion (1 patient), or complex failure with scarring/stricture (6 patients). Nearly all revisions included takedown of prior fundoplication and repair of hiatal hernias. Patients underwent redo-fundoplication (5 patients), Collis gastroplasty and fundoplication (6 patients), primary closure (3 patients), and esophagogastrectomy (4 patients). There were no deaths. Thirteen (72%) had no complications in spite of primarily a left thoracoabdominal approach. Morbidity included aspiration (2 patients), ileus (1 patient), and wound complications (2 patients). The mean hospital stay was 7.3 days [±3.9]. In 10 patients who completed QoL surveys, 8 reported resolution of reflux, 6 reported resolution of regurgitation, while 4 remained on proton-pump inhibitors (PPI). Among those off PPIs, the median time off was 5.5 years [IQR 5,13]. Mean SF36 scores were significantly higher in the study cohort compared to United States (US) norms in four domains: physical functioning (79.5 [±19.9] vs. 50.7 [±14.5], p=0.001), emotional role limitations (83.3 [±36.1] vs. 51.4 [±13.1], p=0.021), emotional well-being (88.4 [±8.7] vs. 54.3 [±13.3], p<0.001), and social functioning (75.2 [±31.0] vs. 51.4 [±15.3], p=0.038). No summary scores were significantly lower than US norms (lower scores indicate greater disability).
Conclusion: Second-time redo anti-reflux surgery through an open approach is safe and effective in relieving reflux symptoms and improving QoL in select patients. The exposure and versatility provided by a left thoracoabdominal approach justifies longer hospital stays, greater post-operative pain, and leads to excellent long-term outcomes.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 93676
Program Number: S082
Presentation Session: Foregut III
Presentation Type: Podium