Justin D Sargent, DO, Steven P Shikiar, MD, John Davis, MD. Hackensack Meridian Health Palisades
INTRODUCTION: There is a wide range of variability in presentation for patients whom ingest foreign bodies (IFB). Most commonly patients are asymptomatic as the foreign body passes through the gastrointestinal tract without any complications. Patients may also present with obstruction, hemorrhage or perforation and subsequent sepsis of any part of the alimentary tract from esophagus to anus. When operative intervention is required traditionally exploratory laparotomy is performed. Here we will present a case of perforating and obstructing IFB treated successfully with laparoscopic bowel resection with intracorporeal anastomosis.
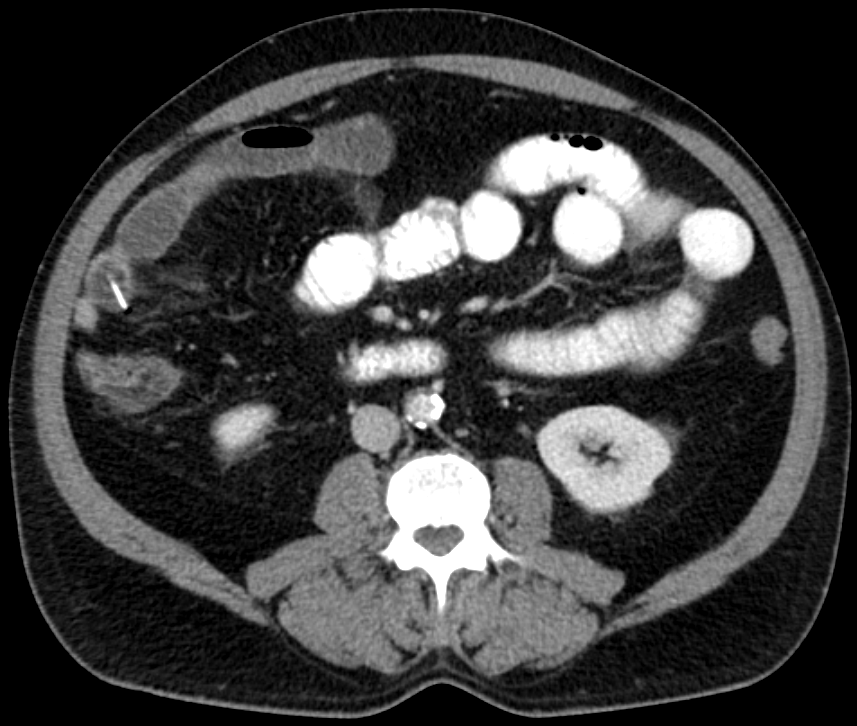
CASE DESCRIPTION: A 67 year-old male, without previous abdominal complaints, presented to the ER with acute onset severe 10/10 sharp, constant, diffuse abdominal pain with associated nausea that began a few hours prior to arrival. Patient had never had any similar symtpoms. No past abdominal surgeries. Palpation of the abdomen showed diffuse tenderness with rebound tenderness in the lower abdomen. Workup was significant for a leukocytosis of 18,300 and CT imaging showing a focal area of small bowel perforation in the RLQ associated with a linear, radiopaque object in the lumen of the bowel at this level with associated bowel obstruction proximally. Further questioning revealed patient had eaten fish 2 days prior without any recollection of swallowing any bones. NG tube was placed and the patient was placed on empirical IV antibiotics and taken to the operating room.
Diagnostic laparoscopy was performed. A loop of small bowel was identified with a small perforation and associated induration of adjacent mesentery. A thin linear object was identified to be protruding from the lumen. Two healthy areas of adjacent bowel were identified. The mesentery to the bowel was divided. The proximal and distal areas of resection were divided with an endo GIA stapler. An intracorporeal bowel anastomosis was performed with the common channel created with an endo GIA stapler. The common enterotomy was closed with 3-0 vicryl in a running fashion. The specimen was removed in through a Pfannenstiel incision. The specimen was then opened on the back table and visualization of the bowel reveled a small linear fish bone with associated ulceration of the mucosa.
Post-operatively the patient had return of bowel function on POD#2, diet was advanced discharged on POD#3.
CONCLUSION: Laparoscopic bowel resection with intracorporeal anastomosis can be a viable option in patients requiring small bowel resection for perforating ingested foreign bodies.

.jpg)
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 94268
Program Number: P027
Presentation Session: Poster Session (Non CME)
Presentation Type: Poster