Richard J Miskimins, MD1, John M Glenn, DO1, Cyril Kamya, MD1, Cole L Paffett, MSIV2, Seyed Arshad, MD1, Edward D Auyang, MD, MS, FACS1. 1UNM Health Science Center, Department of Surgery, 2UNM Health Science Center, School of Medicine
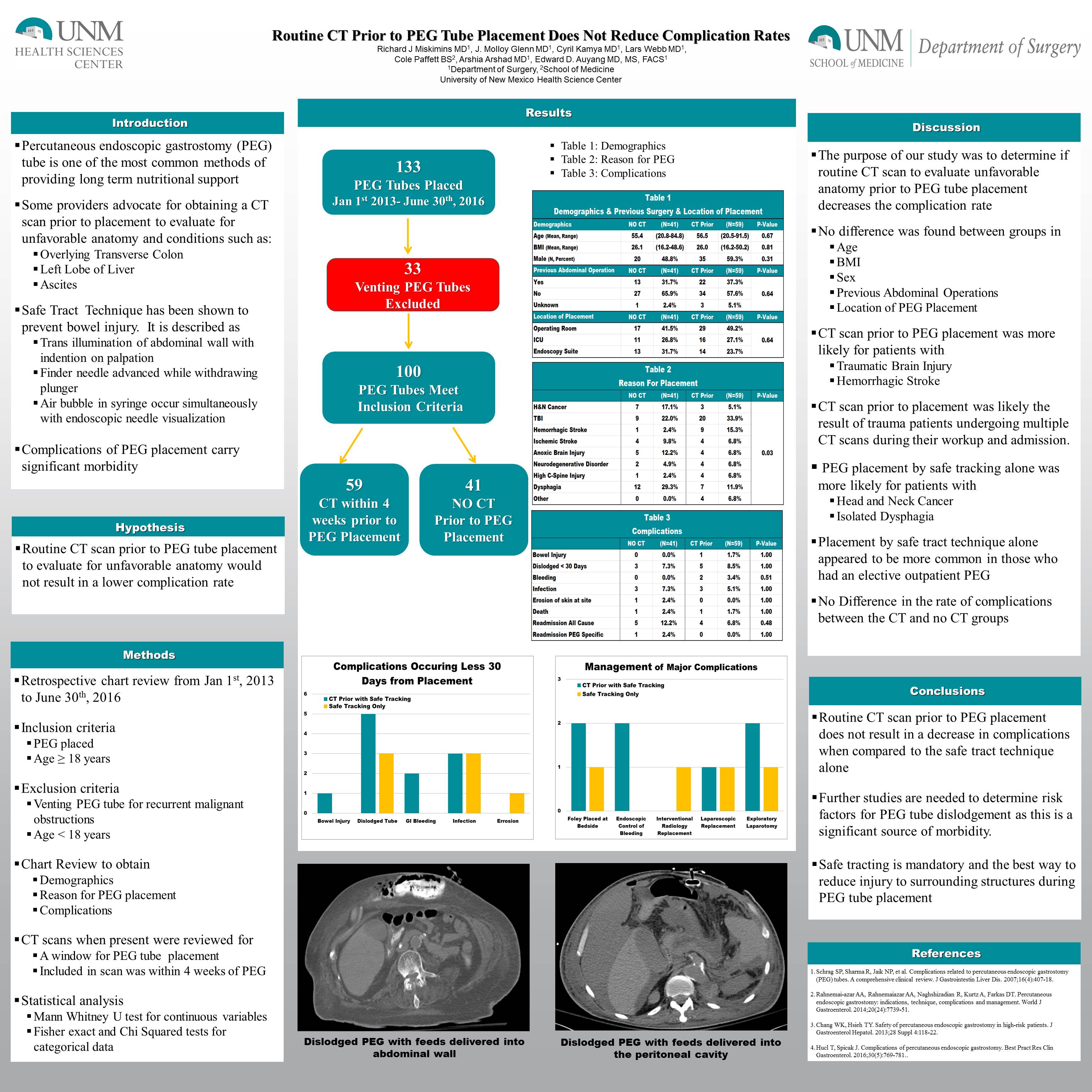
Background: Percutaneous endoscopic gastrostomy (PEG) tube is one of the most common methods of providing long term nutritional support to patients with a functional gastrointestinal tract. Some providers recommend obtaining a CT scan prior to performing PEG to rule out overlying viscera such as the transverse colon or left hepatic lobe. The purpose of our study was to evaluate if CT imaging prior to PEG tube placement resulted in a lower complication rate when compared to transillumination with visualization of the indentation of the operators finger alone.
Methods: A Retrospective chart review was performed on all patients who underwent PEG tube placement between January 1st, 2013 to June 30th, 2016. Those who underwent placement for reasons other than providing nutritional support, such as venting PEG, were excluded. Demographics, BMI, reason for PEG tube placement and if a CT scan was obtained prior to PEG tube placement were extracted. Statistical analysis was performed with Fischer exact test for categorical variables and Mann-Whitney-U Test for continuous variables.
Results: There were 133 patients who underwent PEG tube placement between Jan 1st, 2013 and June 30th, 2016. Of these 22 were venting PEG tubes for malignant bowel obstructions, leaving 111 patients meeting inclusion criteria, 38 patients had a pre-procedure CT (PPCT group) and 73 patients did not have a CT prior to the procedure (NCT group). There were no differences between the groups in regard to sex, BMI, or reason for PEG tube placement. The PPCT group was older (63.7 vs 53.4 years, p<0.01). When the PPCT group was compared to the NCT group there was no difference in the rate of bleeding events (2.6% vs. 0.0% p=0.34), need for operative intervention (2.6% vs. 5.4% p=0.66) and accidental PEG tube dislodgements (5.2% vs 5.4% p=1.0). The NCT group had one injury to a surrounding organ with a PEG tube placed through the colon. It should be noted that the operator in this case failed to transilluminate the abdominal wall prior to puncture.
Conclusion: Routine CT to evaluate for unfavorable anatomy such as overlying liver or transverse colon prior to PEG tube placement does not result in a reduced complication rate. Safe site selection utilizing the correct technique of transillumination of the abdominal wall and visualization of the indentation of the operator’s finger is essential for safe PEG tube placement.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 80791
Program Number: P342
Presentation Session: Poster (Non CME)
Presentation Type: Poster