Kazuo Tanoue, MD PhD FACS, Hidenobu Okino, MD phD, Tomohiko Akahoshi, MD PhD, Yasuhiro Nozoe, MD PhD, Masamitsu kanazawa, MD PhD, Kiishiro Ueno, MD PhD. Ueno Hospital for surgery and gastrointestinal disease
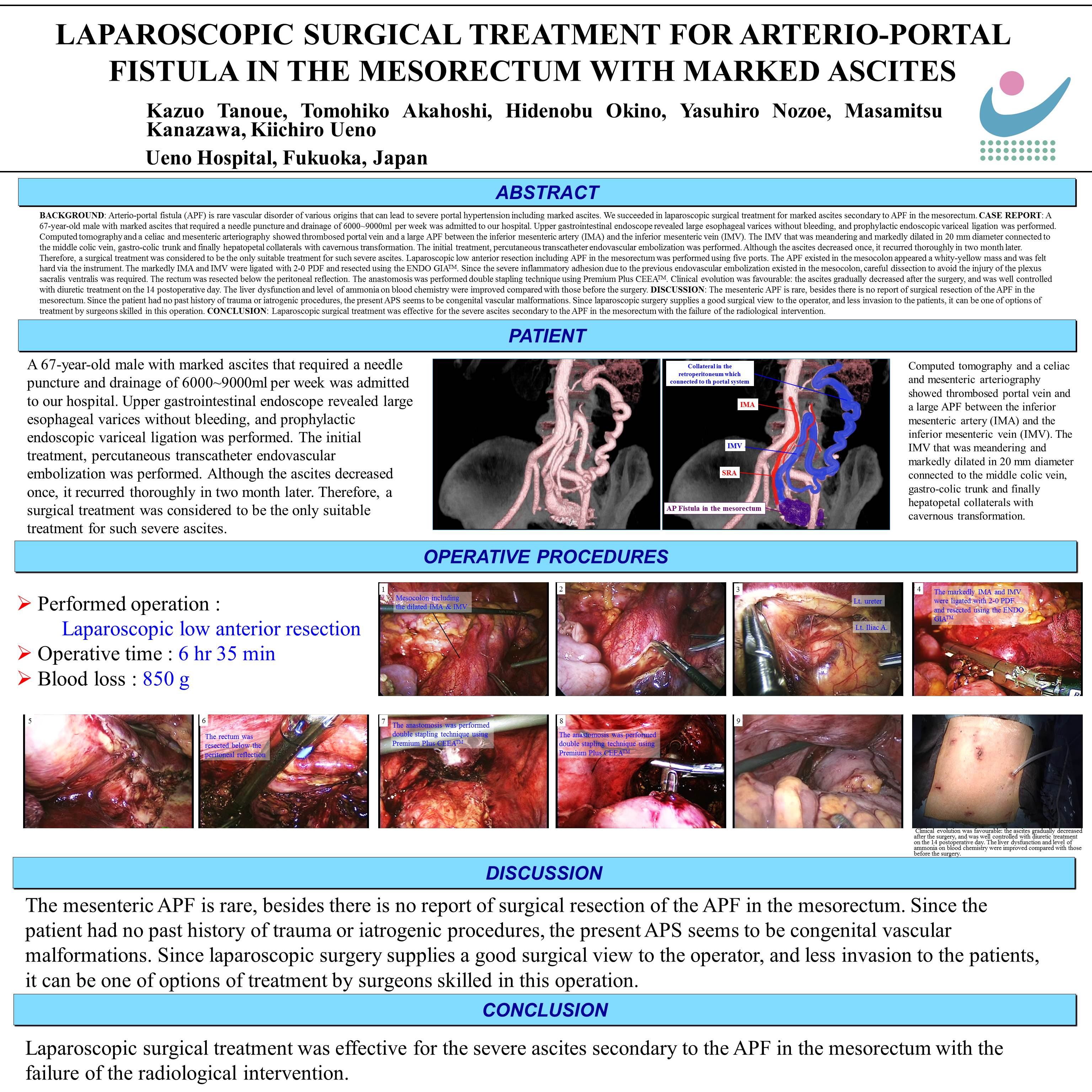
BACKGROUND: Arterio-portal fistula (APF) is rare vascular disorder of various origins that can lead to severe portal hypertension including marked ascites. We succeeded in laparoscopic surgical treatment for marked ascites secondary to APF in the mesorectum.
CASE REPORT: A 67-year-old male with marked ascites that required a needle puncture and drainage of 6000~9000ml per week was admitted to our hospital. Upper gastrointestinal endoscope revealed large esophageal varices without bleeding, and prophylactic endoscopic variceal ligation was performed. Computed tomography and a celiac and mesenteric arteriography showed thrombosed portal vein and a large APF between the inferior mesenteric artery (IMA) and the inferior mesenteric vein (IMV). The IMV that was meandering and markedly dilated in 20 mm diameter connected to the middle colic vein, gastro-colic trunk and finally hepatopetal collaterals with cavernous transformation. The initial treatment, percutaneous transcatheter endovascular embolization was performed. Although the ascites decreased once, it recurred thoroughly in two month later. Therefore, a surgical treatment was considered to be the only suitable treatment for such severe ascites. Laparoscopic low anterior resection including APF in the mesorectum was performed using five ports. The APF existed in the mesocolon appeared a whity-yellow mass and was felt hard via the instrument. The markedly IMA and IMV were ligated with 2-0 PDF and resected using the ENDO GIATM. Since the severe inflammatory adhesion due to the previous endovascular embolization existed in the mesocolon, careful dissection to avoid the injury of the plexus sacralis ventralis was required. The rectum was resected below the peritoneal reflection. The anastomosis was performed double stapling technique using Premium Plus CEEATM. Clinical evolution was favourable: the ascites gradually decreased after the surgery, and was well controlled with diuretic treatment on the 14 postoperative day. The liver dysfunction and level of ammonia on blood chemistry were improved compared with those before the surgery.
DISCUSSION: The mesenteric APF is rare, besides there is no report of surgical resection of the APF in the mesorectum. Since the patient had no past history of trauma or iatrogenic procedures, the present APS seems to be congenital vascular malformations. Since laparoscopic surgery supplies a good surgical view to the operator, and less invasion to the patients, it can be one of options of treatment by surgeons skilled in this operation.
CONCLUSION: Laparoscopic surgical treatment was effective for the severe ascites secondary to the APF in the mesorectum with the failure of the radiological intervention.
Session: Poster
Program Number: P442
View Poster
{kind=link}