Gao L Chen, MD1, Dan Eisenberg, MD, MS2, Eric Kubat, MD2. 1VA Palo Alto Health Care System, 2Stanford University School of Medicine
Background: Obesity is associated with gastroesophageal reflux disease (GERD). Long standing GERD is a risk factor for transformation to Barrett’s Esophagus (BE), a premalignant disease. Although Roux-en-Y gastric bypass is an established treatment of both obesity and GERD, little evidence is available regarding its effect upon BE.
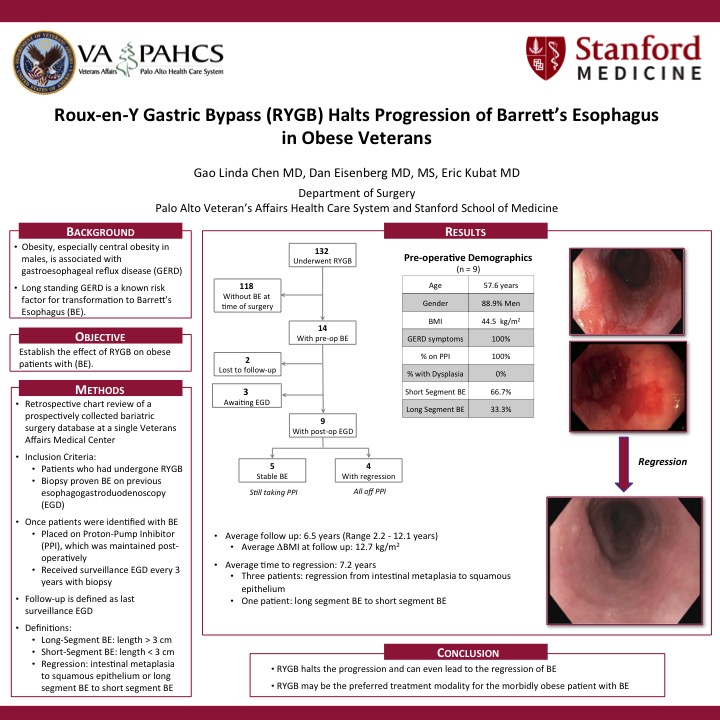
Methods: After IRB approval, Roux-en-Y gastric bypass (RYGB) patients with a preoperative diagnosis of BE were identified and data was abstracted from a prospectively managed bariatric surgery database at an academic-affiliated, Veterans Affairs Medical Center. All RYGB patients underwent a preoperative esophagogastroduodenoscopy (EGD). Patients with biopsy-proven BE received routine surveillance EGD every 3 years. Follow up was defined by last surveillance EGD.
Results: Between 2001 and 2015 bariatric surgery was performed in 287 patients at our institution. 132 bariatric patients underwent RYGB. The incidence of preoperative BE in this cohort was 10.6% (n=14). 11 had short segment BE, 3 had long segment BE; none had dysplasia. Most were men (86%; n=12), the average age was 57 years, and the average preoperative body mass index (BMI) was 45.4 kg/m2. Among the 86% (n=12) of patients who had symptomatic GERD, all were taking a proton pump inhibitor (PPI) preoperatively. One year after RYGB, the cohort’s average BMI decreased to 31.6 kg/m2 and the average percent excess BMI loss (%EBMIL) was 71% (range 36.6% – 97.8%). Two of the 14 patients were lost to follow up, 3 pending surveillance EGD, and 1 patient had BE regression on PPI medication alone prior to surgery. Complete data was available for 8 patients with a median follow up of 85.4 months. Of these, 4 demonstrated regression of BE (intestinal metaplasia to squamous epithelium) and 4 had stable BE with no regression; none had progression of Barrett’s based on EGD with histology. Among patients with BE regression, none required a PPI at last follow-up and among those with stable BE only 2 still required PPI medication.
Conclusion: RYBG can lead to regression of BE in morbidly obese patients with GERD. Most patients experience a decrease in PPI use. Further studies are necessary to determine the role of RYGB in patients with BE with BMI <35 kg/m2.
Presented at the SAGES 2017 Annual Meeting in Houston, TX.
Abstract ID: 79816
Program Number: P010
Presentation Session: Poster of Distinction (Non CME)
Presentation Type: PDIST